
Rethinking Deinstitutionalization: Part I
The Early History of Mental Hospitals

Mental illness has been described in various types of medical literature since antiquity. Hippocrates described both melancholia and mania in his texts, Aphorisms and On the Sacred Disease, stating, “If fear or distress last for a long time, it is a sign of melancholia.” Hippocrates put forth his theory of bodily humors, suggesting melancholia was caused by an accumulation of cold, dry black bile in the brain. Interestingly, Hippocrates noted that loss of appetite, insomnia, irritability, and unprovoked terror were aspects of melancholia. Mania was seen as an acute state caused by yellow bile boiling in the brain or by black bile overheating and creating an aggressive, inflammatory state. In this ancient formulation, mania overlapped with fever and delirium. Importantly, Hippocrates rejected the idea of mental illness as a supernatural phenomenon; hence, the title of his work discounted its “sacred” status.
A surprisingly modern clinical description of mood disorder came in the first century of the common era (CE) from Aretaeus of Cappadocia. Aretaeus published On the Causes and Symptoms of Chronic Diseases, in which he recognized that mania and melancholia were not separate diseases but part of a single biological process. He wrote:
“Melancholia is a part and a commencement of mania. The development of mania is a change toward amplification, rather than a transition to a completely different disease.”
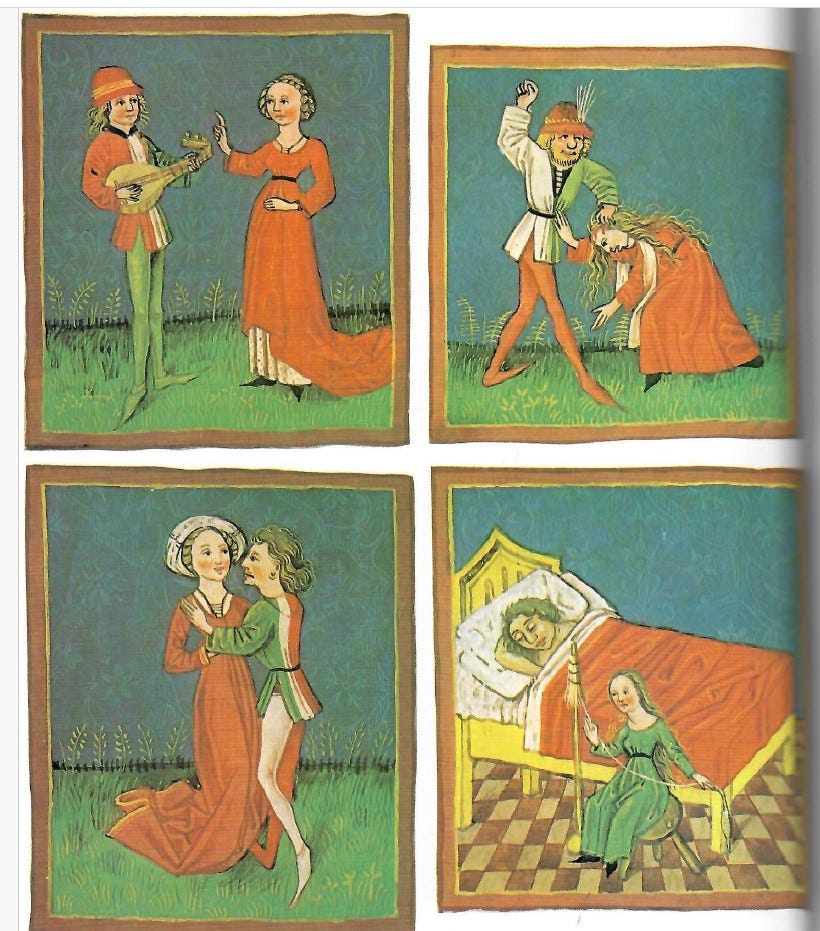
These early descriptions of affective disorder continue in our modern era. The figure below shows an illustration in a medieval medical textbook. The upper left panel is a man singing sad songs, indicating that he suffers from minor depression. The lower left panel shows a man with mania, displaying hypersexuality. On the lower right, a man is bedbound due to melancholia. The hot-blooded, angry man in the upper right panel is abusing his partner. Physicians at that time viewed angry, impulsive people as having dry yellow bile, while the manic individual had too much hot, dry blood. One can see that even at this early time, clinicians struggled with explaining both elated mood and irritable, aggressive behavior.
In contrast to mood disorders, the concept of psychosis evolved much more gradually. Again, Hippocrates rejected demonic possession as a cause for such behavior, but belief in possession as a cause of hallucinations was common well into the 16th and 17th centuries. In one of the first attempts to move away from a “medical model” for mental illness, Heinrich Kramer, the author of the Malleus Maleficarum (”The Hammer of Witches,” 1486), claimed to be able to distinguish between mental illness and witchcraft. His discussion of this issue was highly biased against medical intervention (crude as it was at the time) and pushed the use of exorcism for innocent victims of possession, while witches’ punishment was torture and death.
As rational thinking advanced, the legal system evolved to deal with people with a variety of mental conditions. In 13th-century England, “Lunacy Trials” were held to distinguish between “Idiots” and “Lunatics.” The former were individuals with intellectual disability, while the latter were people born with normal capacity who became mentally ill. Indeed, “lunacy” and “madness” became both lay and clinical terms to describe a wide variety of mental illness. Psychosis was subsumed within these terms. The German physician Karl Friedrich Canstatt first introduced the term “psychosis” in 1841 in his text Handbuch der Medizinischen Klinik. Over the late 19th and early 20th centuries, psychiatrists such as Emil Kraepelin and Karl Jaspers further defined the term and the disorders associated with it, eventually separating it into distinct clinical entities like dementia praecox (schizophrenia) and manic-depressive insanity. The key point is that mental illness, while always influenced by environmental factors, is not simply a label or a product of the culture of a given time. These disorders have been part of the human condition since we evolved. (Please see my video, “What Makes Us Human Puts Us at Risk”).
The Beginning of Hospitals for the Mentally Ill
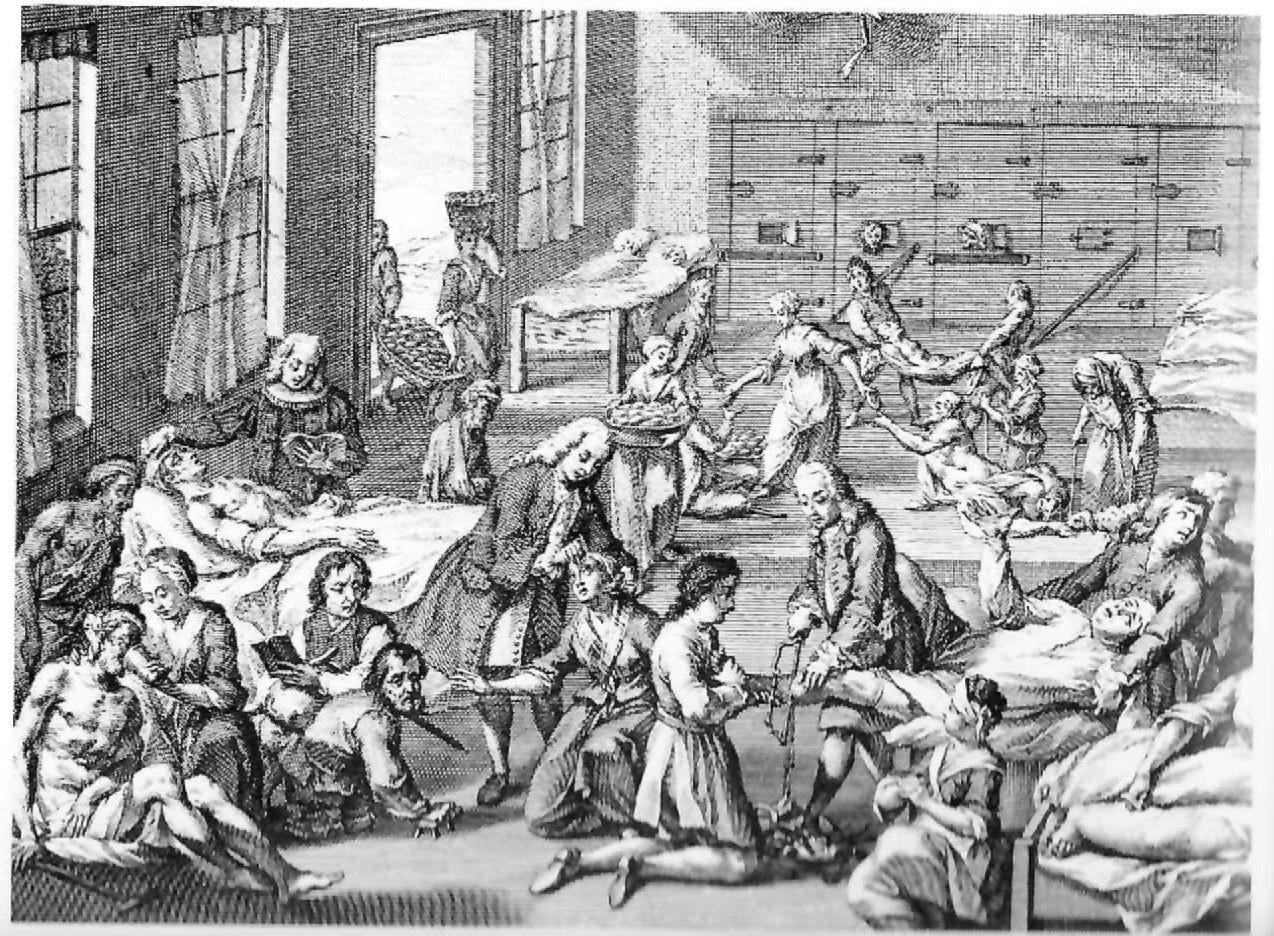
If you visited any type of hospital before the invention of sterile techniques and anesthesia, it would be a scene of unrequited horror. Amputations were performed on awake patients with no painkillers. Surgeons sawed through the bone while the patient screamed and attendants held them down. Surgery was so brutal and surgeons had such limited training that in Great Britain, they were not allowed to use the title “doctor,” a tradition that exists in the UK to this day. The figure below shows hospital medicine in Hamburg, Germany, in the 18th century. Notice the amputation and eye surgery going on in the middle of the ward. A patient to the left is being given last rites while mentally ill individuals stare out from their cell doors and manic patients dance. The point here is that all of medicine was barbaric during this era, and treatment of the mentally ill was neither worse nor better than treatment of people with other diseases.
The Bethlem Royal Hospital (“Bedlam”) in London was noted to be admitting mentally ill people as early as 1377. In 1815, after a series of scandals, the hospital moved to the Southwark area of London into a new building. Medical oversight was improved, and public viewing of people with mental illness for entertainment was banned. Such viewing was deemed inhumane for the rest of the 19th and 20th centuries, only to be revived on social media in the last decade!
The Enlightenment inspired the American and French revolutions. As noted in the introductory essay, Virginia had already established a hospital for mentally ill people before the foundation of the United States. The late 18th and early 19th centuries were periods of great optimism that improving the physical and spiritual conditions of people could cure mental illness. Among the most famous of this generation of physicians was Philippe Pinel, director of the Salpêtrière hospital in Paris, which at that time had over 8,000 patients. One in ten of these patients was being treated as a “lunatic” and most were considered beyond help. As shown below, Pinel is best known for un-shackling the insane, although Pinel himself did not write about doing so, and the process of unchaining may have begun before he arrived at the Salpêtrière. (The painting was done by Tony Robert-Fleury in 1876.) However, his contributions to the field of mental health were significant in other areas as well.

Moral Treatment and its Successors
Most histories of state hospitals tend to focus on the period immediately before the onset of deinstitutionalization. Many of these histories are written by people with a frank anti-psychiatry bias. Even books that attempt to more objectively describe the history of psychiatry regard the era of state hospitals as a dark age where little value was accomplished. State hospitals are viewed at best as an example of good intentions gone bad. This is far too simplistic a view. This series on rethinking institutionalism will not shy away from many of the problems of institutional care in the late 19th and early 20th centuries. It will, however, seek to puncture the myth that callous forces imprisoned the mentally ill in state hospitals. We will look at some of the underlying reasons for the massive increase in census that these hospitals experienced by the beginning of the 20th century.
Little known to most mental health clinicians, Gerald N. Grob (1931-2015) was a prominent historian of American mental health care policy and medicine. His Wikipedia page lists his many works on these topics; three of his books were very valuable for this project. Grob documented the creation of state hospitals from colonial times through the 19th century in his first book, Mental Institutions in American: Social Policy to 1875. The second book, Mental Illness and American Society, 1875-1940 documented the crisis in mental health care as state hospital populations increased from 1875 to 1940. Finally, Grob examined the deinstitutionalization movement in his book, From Asylum to Community. What makes Grob’s work particularly valuable is his discussion of many source documents describing the progress and debates about mental health care in America. He obtained access to some extraordinary statistical data about the state hospital patients of the 19th and early 20th centuries that may change your view of these institutions. Another invaluable resource was E. Fuller Torrey’s American Psychosis, published in 2014, in which he examined the politics and cynical maneuverings of the deinstitutionalization movement.
Returning to Philippe Pinel, he contributed to the classification of mental illness, recognizing the major categories as melancholia, mania with and without delirium (Pinel likely used this term to refer to psychosis), dementia, and “idiotism” (intellectual disability). Along with other physicians in Europe, he pioneered the use of statistics in medicine. His Moral Treatment quickly spread to America, where it was endorsed by many of the Founding Fathers, including the Hancock family, Benjamin Franklin, and Benjamin Rush (the latter being regarded as the father of American psychiatry). Moral Treatment often discarded the prevailing practices of the time—such as bleeding, purging, spinning chairs, and indefinite chaining—in favor of a structured, psychological intervention. Pinel was among the first to formally argue that mental “alienation” was often triggered by intense emotional distress or environmental trauma. (By ending the purging and bleeding of the time, Pinel likely improved the health of his patients just by doing no harm.) Pinel was clear, however, that structure was needed for the mentally ill to improve, and patients had to adhere to clinical authority.
Even before the 1776 Revolution, American cities were beginning to struggle with the presence of both mentally ill individuals and impoverished people. Large colonial cities established what were referred to as “almshouses” to care for destitute people. People of that era struggled to define the difference between the “deserving poor” and those who are simply unwilling to work. It became clear that many mentally ill individuals were residents of these almshouses. Grob quotes a committee of citizens in 1790 Boston who wrote:
“The almshouse in Boston is perhaps the only instance known where persons of every description and disease are lodged under the same roof and in some instances in the same contagious apartments, by which means the sick are disturbed by the noises of the healthy, and the infirm rendered liable to the vices and diseases of the diseased, and the profligate.”
Philadelphia Hospital (founded in 1751) was known for treating the mentally ill. Benjamin Rush practiced there for 30 years, being distressed at the frequent use of “mad shirts” or “straitjackets.” From the 1770s to the 1820s, these mental hospitals were small or privately run, but by the 1840s, the number of mentally ill people needing help began to grow.
State Hospitals Emerge
Horace Mann (1796-1859), later known for his educational reforms, was instrumental in passing legislation establishing the first mental hospital in Massachusetts in 1830. Samuel B. Woodward was superintendent of the Worcester State Lunatic Hospital from 1833 to 1846. Woodward was the first president of the Association of Medical Superintendents of American Institutions for the Insane (now the American Psychiatric Association). The person most associated with the expansion of American State Hospitals is Dorothea Dix (1802–1887). Her crusade on behalf of the mentally ill began in Cambridge, Massachusetts, in 1841, when she was asked to teach a Sunday school class to criminals at the local jail. She was shocked to find a group of insane individuals confined alongside the criminals. Ultimately, Dix was responsible for founding or enlarging over 30 mental hospitals in the United States and in other countries. Moreover, she pressed for a greater role of government in the care of the mentally ill. Dix was able to persuade Congress to pass a bill setting aside federal land to support asylums for the mentally ill, but President Franklin Pierce vetoed it.
As Grob describes in his first book, these early institutions were intended to be small, often with no more than 100 to 200 patients. There was enormous optimism about the possible benefits of Moral Treatment. Hospitals were set in rural areas and often were nearly self-sufficient from farming or keeping livestock. Patients were encouraged to engage in these activities as a kind of early occupational therapy. There was early debate about the role of physicians in the care of the mentally ill. The term “psychiatry” was coined in 1808 by the German physician Johann Christian Reil, and Benjamin Rush is said to have published the first American textbook on mental illness in 1812. Physicians at these early state hospitals had only general medical training and learned from informal experience. (Adolf Meyer is credited with establishing the first formal training program in psychiatry at Johns Hopkins University in 1910.)
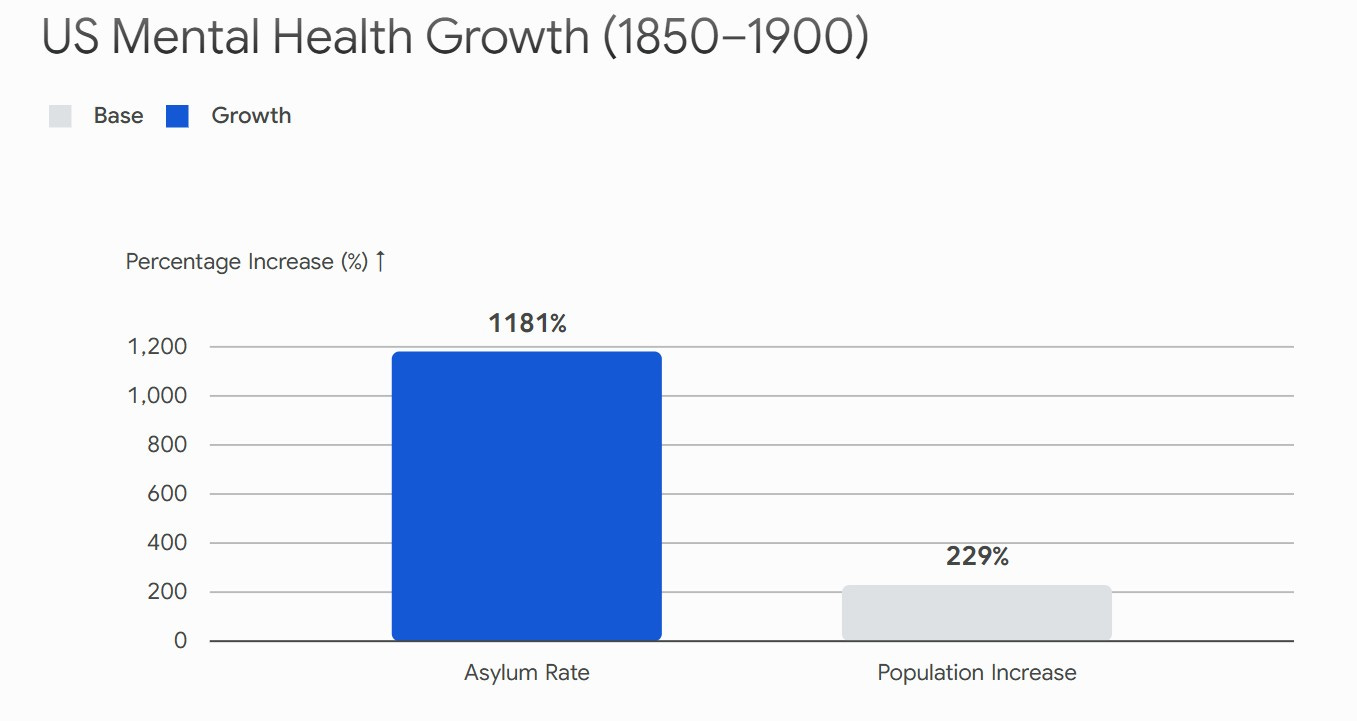
Almost immediately, these young institutions were overwhelmed by admissions. Moreover, while it was initially assumed that most patients would be successfully treated and released, the number of chronic patients continued to rise. As Grob documents, there was enormous tension between the state hospitals and local communities over the appropriateness of various types of admissions. Superintendents objected to the admission of “chronic” and “destitute individuals” who would be unlikely to benefit. The graph below shows the enormous increase in the number of people in state hospitals over the period from 1850 to 1900. While the population of the US increased by about 230% over this period, the number of people institutionalized for mental illness rose by over a thousand percent.
What was the cause of this increase? There have been two major theories put forward over the last several decades. One is the “Recency Hypothesis,” which suggests that mental illness in general and psychosis in particular became more common in the population. The other is the “Social-Control Theory,” which argues that in the late 19th century, society became intolerant of the mentally ill and of behavioral differences in general. This allegedly resulted in communities transferring these individuals to state institutions. As to the Recency Hypothesis, it does appear, as noted earlier, that psychotic symptoms were less commonly noted by physicians prior to the 19th century. This may have been simply because they were subsumed under the general term of “lunacy.” Nonetheless, the writings of clinicians of the time clearly showed that they were dealing with a new and unexpected phenomenon. Edward Jarvis, one of the founders of what would become the APA, authored the influential 1852 essay On the Supposed Increase of Insanity. He concluded that the spike in severe psychiatric presentations was not an illusion of better record-keeping, but a biological reaction to modern life:
“Insanity is then a part of the price we pay for civilization. The causes of the one increase with the developments and results of the other. [...] In this opinion all agree. [...] [There are] more opportunities and rewards for great and excessive mental action, more uncertain and hazardous employments and consequently more disappointments... and more painful struggles to achieve that which is beyond reach, or to effect the impossible.” (American Journal of Insanity [now Psychiatry] 8:333-364)
A complete critique of the Recency Hypothesis is beyond the scope of this article. It is known that migration, prenatal malnutrition, urban living, and obstetrical complications are all risk factors for schizophrenia. These factors increased markedly in the 19th century. Irish immigrants to America in the 1840s and 1850s were seriously impacted by the first three of these factors. Grob’s publication of documents contain comments from hospital superintendents in the US about the large number of mentally ill immigrants in their facilities. The psychiatrist David Healy and colleagues have written that toxic urban environments due to the Industrial Revolution may have increased the vulnerability of the population to psychosis. Finally, it has been suggested that improvements in obstetrical care in the late 19th century made it more likely that compromised infants would survive, thus increasing the percentage of the population possibly vulnerable to psychosis. This hypothesis remains hotly contested, as some studies show that with proper analysis, there in fact has been no change in the prevalence of schizophrenia over the last 150 years.
The Social-Control Theory was articulated by Michel Foucault in the 1960s-1970s and more recently (and in a more refined form) by Andrew Scull (2015). In 1965, Foucault published Madness and Civilization: A History of Insanity in the Age of Reason, which was his core text for his “Great Confinement” thesis of why asylums emerged. Foucault argued that in the 17th to 19th centuries, Western governments undertook deliberate efforts to institutionalize deviance of all sorts, including the mentally ill, the poor, and the idle. His argument, which would become a foundational principle of the deinstitutionalization movement, was that the hospital was less about treatment and more about imposing state norms, surveillance, and discipline. Scull’s version of the Social Control Theory is more empirically grounded and less conspiratorial. Scull argues that industrialization, urbanization, and the breakdown of traditional family structures created a need to manage difficult populations. In his book, Museums of Madness, Scull appears to acknowledge the reality of mental illness but has a very dim view of psychiatric treatments. He argues that the rise of psychiatry and state bureaucracies occurred due to the need to sustain asylum expansion. While his book is beautifully written as a historical overview, his theme is that psychiatry did not provide any benefit in the past and thus current treatments (i.e., psychopharmacology) do not either and are part of the same system of social control.
The Social Control Theory provided major impetus to the deinstitutionalization movement. After all, if the hospitals were there merely to control the disadvantaged and for the professional and financial benefit of those who ran them, then getting rid of hospitals will do no harm and indeed is a moral imperative. What is completely inconsistent with the Social Control Theory is how little evidence there is for it in the statements and writings of the people running state hospitals at the time. Here is a section of the 1889 bill that established the San Antonio State Hospital:
“The fact that there is a large number of insane persons in the jail of the state who are in need of immediate treatment, creates an emergency, and an imperative public necessity exists requiring the suspension of the constitutional rule which requires bills to be read on three several days in each house, said rule is hereby suspended, and that this act shall take effect and be in force from and after is its passage, and it is so enacted.”
The point here is mentally ill people were already in jail; they were not peacefully living with their families in some rural paradise. Dorothea Dix and her associates were responding to a problem, not trying to create one for the benefit of the psychiatric profession. When the San Antonio State Hospital opened in 1894, the local newspaper wrote enthusiastically of the facility:
From the San Antonio Daily Express (August 26, 1894): “Instead of finding the patients confined to narrow cells, they are allowed to roam at will throughout broad corridors and halls with regular outings twice a day. Instead of brutal turnkeys, there are a number of uniformly courteous, polite, and considerate inmates.”
W. L. Barker, the hospital superintendent, went to great lengths in the article to explain the extensive training the staff received.
“It is a peculiar fact that their [the patients’] violence is soon curbed here. If we get a violent patient one day, as a general thing he is practically quiet the next. The reason I assigned for this, principally, is because we have assistants who are thoroughly trained. They know when to humor a patient and vice versa, and the consequence is that they quickly get the patient under control… There is no necessity for severe treatment as there are better and more humane methods by which these poor people can be made to restrain themselves.”
It would be hard to find a better description of de-escalation techniques for working with agitated inpatients in our own time. These are not the views of people seeking to confine and dominate the disadvantaged.
Another strong argument against the Social Control Theory is the enormous angst of 19th-century hospital superintendents who struggled with overcrowded wards, constant demands from the community to admit more patients, and the refusal to accept discharged patients back into the community. Chapter V of Grob’s book, Mental Institutions in America, contains multiple testimonies from psychiatrists and hospital superintendents about the need for hospitals to have a modest census and of the dangers of overcrowding. But the hospital censuses kept growing. Was this society’s demand for “social control” or something else? Grob writes:
“As long as hospitals remained small, superintendents were able to supervise personally the care of their patients and conduct routine administrative duties as well… But as institutions grew in size and the nature of the patient body changed, superintendents found it increasingly difficult to meet both these responsibilities. No longer were they able to run their institutions in a loose and informal manner. With three, four, and 500 patients the problems of social organization and adjustment were far more complex. The heterogeneous nature of the patient population merely compounded the problems arising out of growth, for each category of inmates seemed to require a different type of care and treatment. The needs of older patients, of chronic patients, of patients suffering from a somatic form of disease, of insane criminals, of alcoholics, and of patients amendable to therapy all differed sharply in many respects and often proved antagonistic or irreconcilable with each other.”
By the late 19th century, state hospital superintendents found themselves overwhelmed with two particularly intractable groups of patients. This would significantly increase hospital censuses and lead to state hospitals with thousands of patients by the 1940s. Who were these patients? I shall answer this question in Part II.
Grob, C. N. (1983). Mental Illness and Society, 1875-1940. Princeton, New Jersey: Princeton University Press.
Grob, C. N. (1991). From Asylum to Community: Mental Health Policy in Modern America. Princeton, New Jersey: Princeton University Press.
Grob, C. N. (2009). Mental Institutions in America: Social Policy to 1875. New York: Free Press.
Redmond, F.C. (2006) History of Psychiatry in Bexar County ISBN 0-61513334-7
Scull, A. (2015). Madness and Civilization: A Cultural History of Insanity. Princeton, New Jersey: Princeton University Press.
Dr. Pliszka: Excellent article with much depth. Thanks as always!
Ashok
Steven, the scale problem may be the most clarifying thread here. The early asylum was not a smaller version of the state hospital. At a human size, routine and personal knowledge could still function as care, because the place could know a patient closely enough for structure to be therapeutic.
Past a certain census, the same tools quietly changed jobs. What had been supervision turned into administration, and the routine that once steadied a patient became a form of containment. A place built to return people to ordinary life slid into a machine for holding the ones the world would not take back. That makes the history harder than either benevolence or social control, and more useful: a humane idea can fail by being asked to work at a scale where the conditions that made it humane no longer hold.