
Re-thinking Deinstitutionalization: A Preview

Suppose that in the period 1950-1970, it had been decided by consensus among elites that cancer was not a biological illness. What if our thinking about cancer evolved like so:
“We have been viewing cancer too narrowly by using a medical model (today, we would say through a medical “lens”). We now see that cancer is caused by social problems and that it is a label we use due to our narrow view of what constitutes health. Worse, we have been using medications to merely treat the “symptoms” of cancer instead of looking at its “underlying” causes. These anti-cancer medications have terrible side effects: they cause people to vomit, lose their hair, suppress their immune system and develop infections. We have not balanced the risks and benefits of treatment. In the 1950’s, the survival rate of most cancers was not that good, even with treatment. Also, we put people with cancer into “institutions” (hospitals) and took them out of their community. It became obvious what the solution is. We need to discourage the use of chemotherapy and radiation and focus on the “root’ causes of cancer (chemicals in environments, poverty) and we need to close the cancer hospitals so people can return to the community. Once freed from the repressive medical model, they will flourish.”
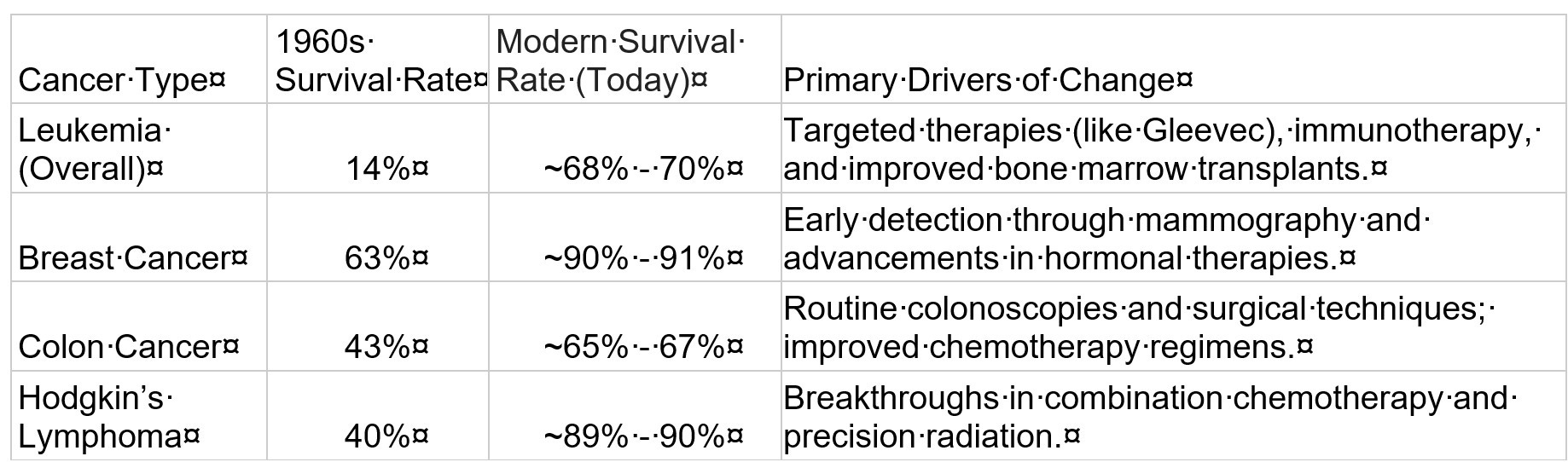
Such a proposal would have struck people as ludicrous. Of course, treating cancer as a biological phenomenon has led to massive advances in the understanding of its causes and a dramatic improvement in survival rates for many common cancers over the last several decades:
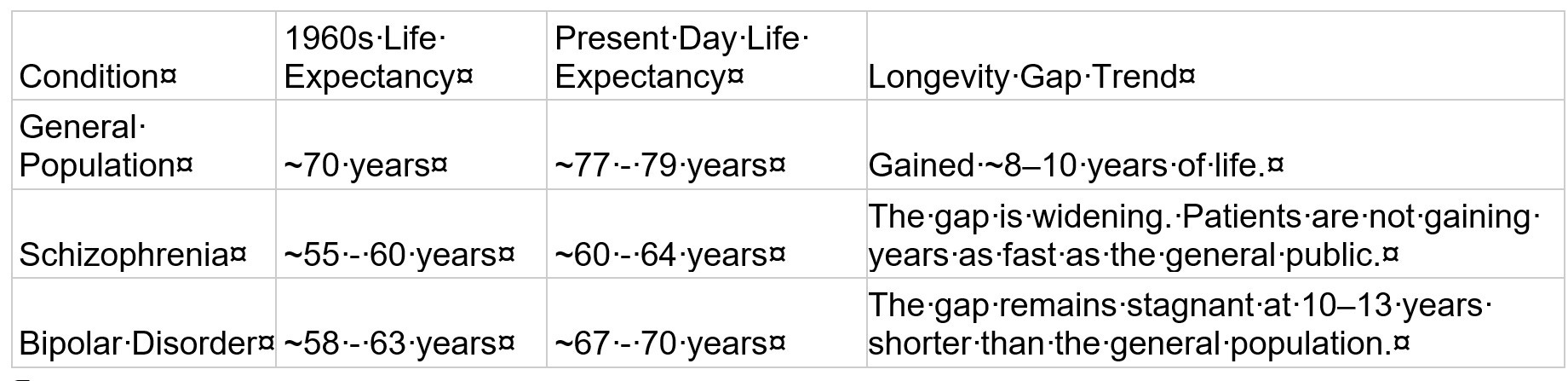
In contrast, while there have been advances in the treatment of mental disorders over the last six decades, the gap in life expectancy for people with severe mental disorders and the general public has widened during this time:
Most people may know that many state hospitals were closed or had their census reduced in the period from 1960 to 1980 due to the policy of deinstitutionalization. Under this policy, individuals with mental illness were to transition from long-stay psychiatric hospitalization to community-based care. This story, however, is often told too narrowly about community-based care not being adequately funded after patients were discharged, leading to homelessness and incarceration. There is a bigger issue with deinstitutionalization than the mere lack of funding. The deeper problem of deinstitutionalization was the emergence of a false narrative as to the nature of mental illness itself. An ideology emerged that mental illness was either the product solely of society’s injustices or not a real entity. Psychiatric diagnoses were ridiculed and dismissed, and psychiatric treatments were disparaged. Oddly, much of this was done in the name of “de-stigmatizing” mental illness but had the end result of creating more stigma. Our cities are now full of the homeless mentally ill, mass shootings perpetrated by individuals with mental illness are a too common occurrence in the US, and deaths from substance abuse (despite recent minor declines) remain at historic highs.
This is a complex problem with many moving parts. In the coming months, I will be rolling out the “Re- Deinstitutionalization,” a five-part series to explore how this problem came about. It is partly a story of good intentions gone awry but also bad intentions that accomplished exactly what was intended. The series will cover:
Part I: Early History of State Hospitals: How they Came About
The people of 18th- and 19th-century America would have been very familiar with our current dilemma. Already at that time, the problem of how to deal with serious mental illness was a major problem in colonial America. In 1766, Francis Fauquier, the Lieutenant Governor of Virginia told the House of Burgesses:
“It is expedient I should also recommend to your Consideration and Humanity a poor unhappy set of People who are deprived of their senses and wander about the Country, terrifying the Rest of their fellow creatures. A legal Confinement, and proper Provision, ought to be appointed for these miserable Objects, who cannot help themselves. Every civilized Country has a Hospital for these People, where they are confined, maintained and attended by able Physicians, to endeavor to restore to them their lost reason.”
Things moved slowly (perhaps distracted by the Stamp Act, among other things) and then on July 6, 1769, a man named Charles Thompson was murdered by his wife who was known to be mentally ill. Like the deaths of the married couple Rob Reiner and Michele Singer in our time, this shocked the community and the local paper opined:
“It is really shocking to see the number of miserable people who have left the use of their reason, that are daily wondering about, for want of a proper house to keep them confined in. If there had been such a place, this poor man would not have met with the above untimely end.”
As a result, a “Public Hospital,” caring for all Virginians suffering from mental illness was established; it became Eastern State Hospital, which exists to this day. The early history of the creation of state hospitals is an important one, as both medical professionals and the political leadership of many communities were truly inspired to improve the lives of the mentally ill and were, in many ways, clearer minded about the challenge of mental illness than we are today.
Part II: Reexamining the “Snake Pit”
How bad did state hospitals become by the early twentieth century? There is no doubt that state hospitals faced the problem of overcrowding and deteriorating infrastructure, but why was this? In popular telling, the state hospitals became warehouses for disadvantaged people, and it was the hospital itself that caused institutionalization. That is, the patient deteriorated because they were confined in the hospital, particularly in the “back-wards.” Movies such as One Flew Over the Cuckoo’s Nest, released in 1975 and based on the 1962 novel of the same name by Ken Kesey, did much to cement the public’s negative view of mental institutions in general. The author, Ken Kesey, intended the movie to be symbolic as a critique of authoritarianism, though Kensey was certainly anti-psychiatry himself. The novel and film convinced many that electroconvulsive treatment and even hospitals themselves were simply punishments for “different” or non-conformist people. By the 1960’s, state hospitals were often overcrowded and not fully therapeutic, but it is important to understand why. The answers will surprise you.
Part III: A “Right to be Mentally Ill?” The Legal Quagmire of Deinstitutionalization
Many trends led to deinstitutionalization, but a major force was the change in the legal landscape regarding involuntary hospitalization and the treatment of the mentally ill that emerged in the 1970’s. The earlier phase of deinstitutionalization was driven by public sentiment and a consensus among mental health professionals that community treatment was better. However, the complete shuttering of state hospitals and the inability of communities to require inpatient care for those who need it was cemented by a series of court decisions that moved the process of involuntary treatment from a “medical model” (where doctors decide) to a “legal model” (where judges decide based on dangerousness). We could rebuild all the psychiatric residential facilities needed for treatment, but we still might not be able to effectively intervene for many patients due to these problematic decisions. We will look at them (O’Connor vs. Donaldson, Addington vs. Texas, Lessard vs. Schmidt, Rennie vs. Klein) in detail and ask whether they were, in legal parlance, “wrongly decided.”
Part IV: The Deadly Consensus: How the Left and the Right Abandoned the Mentally Ill
In her book, The March of Folly from Troy to Vietnam, the historian Barbara Tuchman, wrote of disastrous policies followed by governments both ancient and modern. In the preface of her book, Tuchman defined “folly” as follows: the policy was against the self-interest of the society, it was not the fault of an individual but of a group (“Group think, in today’s lingo), it was not the only policy option to solve the problem, and it was pursued despite worries that it was a mistake or in the face of evidence that the policy was failing.
Community treatment of the mentally ill was assumed by liberal/progressive people of the 1960’s to be a policy that would painlessly work. New psychoanalytically- oriented treatments would cure most people with mental illness and new programs to achieve social justice and redistribution of wealth would eliminate all forms of mental illness. There were extremists such as Thomas Szasz who claimed mental illness did not exist at all. Most on the left did not go that far, but the idea that society just needed to be more tolerant of people who were different became widespread.
In the first part of the 20th century, state hospitals were often the largest component of the budget for most states. In the 1960’s, deinstitutionalization shifted costs away from states onto the federal government and local government (through the creation of Social Security Income [SSI] for the mentally disabled and Medicaid to fund local programs for the mentally ill.) Many progressives assumed “money would follow the person” and a flood of state and federal money would support the new community health movement. For a short time this occurred. In 1980, Jimmy Carter signed the Mental Health Systems Act of 1981 to increase funding for Community Mental Health Centers. However, the Omnibus Budget Reconciliation Act (OBRA) of 1981, Ronald Reagan’s first major piece of legislation, repealed Carter’s Act and converted funding into block grants for the states with an immediate 25-40% cut in funds. While more funds have flowed into the block grants since 2000 (and especially since COVID), it is not clear that services have expanded adequately or that we have the right kind of services. Thus, abandonment of the mentally ill is a sad testimony to rigid ideology on both sides of the political spectrum.
Part V: From the “Least Restrictive Environment” to the “Most Therapeutic Environment”
Where do we go from here? I am not calling for the re-establishment of the state hospitals of yesteryear with their tens of thousands of patients. There is a need for a “vertically integrated” system of in-home care, outpatient care, mandatory participation in treatment (such as Assertive Community Treatment), residential care, and for a small subset of seriously ill individuals, state hospital care in secure settings. This is a daunting task, but the biggest hurdle is intellectual. Can we get past the notion that treatment of mental illness is a denial of liberty when in fact it is liberating? The final part of this series will look at designs of treatment systems that restore the individual to their full potential in the community. This, after all, was the original goal of “community mental health.”
Part I should be out in mid-June 2026