


Do Psychiatric Medications Prevent Violence?
In Almost All Cases, Yes

In my most recent post, I discussed the prevalence of serious mental illness among the small number of persons who have committed mass shootings. I also pointed out that most of these individuals received no or inadequate treatment for their mental illness, begging the obvious question as to whether early treatment would have prevented their tragic acts. Mental health professionals take this as a given, though there might be disagreement about what type of treatment would have been most effective (medication vs therapy vs wraparound services, etc.). Recent polls, however, show that some in the lay public do not share this view. A Gallup survey conducted in May 2024 showed that while cost is viewed as a major barrier to people in seeking mental health care, 24% of adults felt that treatment would not help and 28% felt that mental health conditions can be handled on their own. While half of the survey participants (53%) saw therapy as helpful, only 35% felt psychiatric medication was helpful.
“The Prozac Defense” arose in the 1990’s as people accused of violent crime alleged that fluoxetine induced their behavior; most of these cases were unsuccessful with some notable recent exceptions. The current Health and Human Services Secretary nominee has a history of linking antidepressant drugs to violence:
It is likely that the issue of psychiatric medications and violence will be in the public eye with much higher stakes for our patients. It is therefore critical to look at the whole of the literature in this area. Let us start with mass shootings and then look at larger epidemiological studies which can address the issue more fully. In 2019, Ryan Chaloner Winton Hall and colleagues sought to ascertain how many school shooters had been on psychiatric medication either at the time of their crime or in their past. They examined FBI reports, news sources with citations, and other official reports of 49 separate incidents. Twenty-three (47%) of the shooters had a history of being prescribed psychiatric medication, but none had been to a psychiatric provider (as best could be determined) in the three months prior to their acts. Peter Langman reviewed many school shooting cases and found that only 12.5% of the shooters had a psychiatric medication history and that most often, their troubled behavior preceded their psychopharmacological treatment. Langman also noted that many social media reports are simply wrong or fabricated altogether:
“After the Sandy Hook Elementary School shooting, Adam Lanza was believed by some to have been taking psychiatric medication. This was partly due to a man purporting to be his uncle claiming that Lanza was taking an anti-psychotic drug called Fanapt. As it turned out, the man was not Lanza’s uncle; he was subsequently arrested for violating his probation related to conspiracy and wire fraud charges. The report that Lanza was taking Fanapt was a complete fabrication.” (pg. 5)
Bear in mind that it is probably more striking that there was not a higher rate of psychiatric medication prescribed in these individuals, at least in those who had documented histories of mental illness. If one surveyed a group of patients who had seizures, one would likely find that most were or had been prescribed anti-convulsant medications at some point. If a person with a seizure disorder stopped or only took their anti-convulsant medication intermittently, we would not be surprised if they suffered a seizure. If we apply the same reasoning to people who commit irrational acts of violence, we could hypothesize that it was the lack of psychiatric medication that may have contributed to these acts.
In my post on the effects of social media on youth mental health, we reviewed the difficulties in trying to determine if the rise in suicide was caused by the increase in social media usage, even though the two were highly correlated. For any discussion of the role of psychiatric medications in violence, we have a strong counterfactual: As psychiatric prescribing for children has increased over the last several decades, violent crime among juveniles has been decreasing:
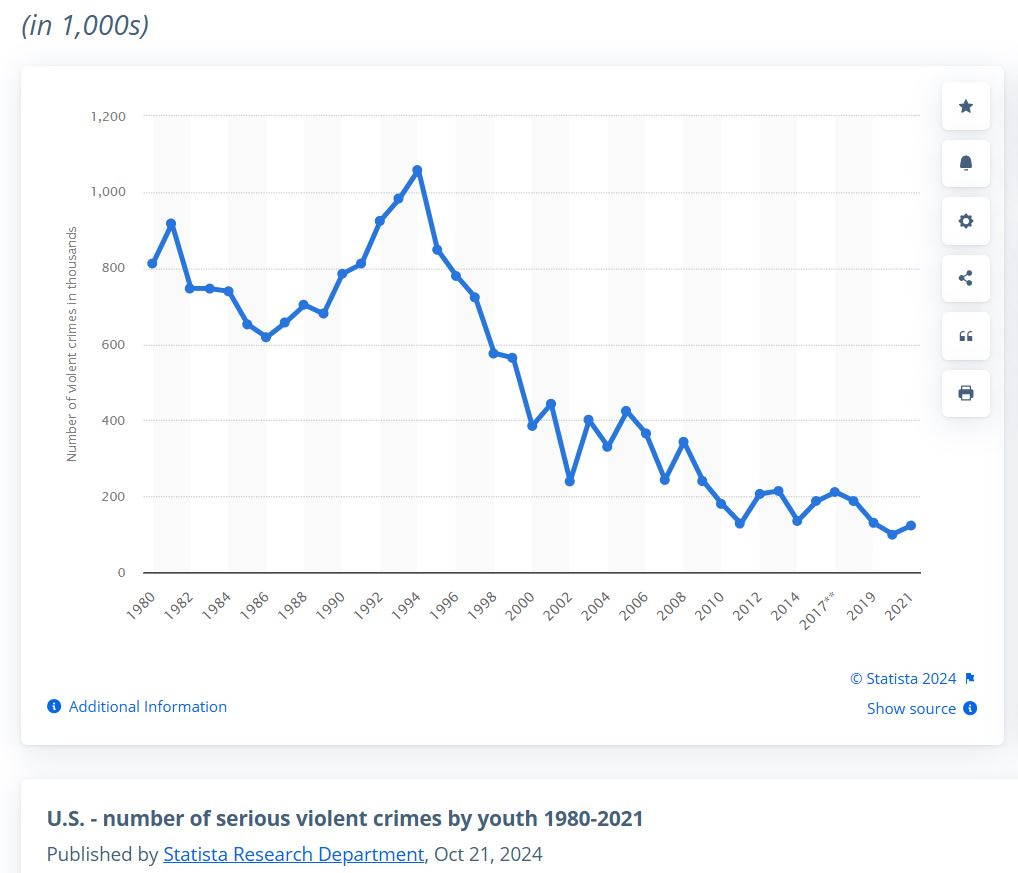
Are you shocked by the above data? Of course, these are nationwide figures. Individual cities, particularly during and after the pandemic, have had increases in juvenile crime. News about juvenile crime often rises to the top of the news and social media feeds. While increases in the rate of prescriptions of psychiatric medication for youth is sometimes portrayed as being an epidemic in itself, the truth is far more nuanced. Yasir Altuwairqi reviewed worldwide studies on the prevalence of the use of psychiatric medications from 2013 to 2023. He noted the variation in these rates:
“Stimulants showed a consistent prevalence rate over the years. Antidepressants, including selective serotonin reuptake inhibitors, have demonstrated variations over the years, with a substantial increase in 2015, followed by a decrease in subsequent years. In addition, antipsychotics, including atypical antipsychotics, have varied over the years; however, their use increased in 2023. Anticonvulsants and anxiolytics were also utilized, albeit at lower prevalence rates.”
Maria Tcherni-Buzzeo of the University of New Haven explored factors in the fall of juvenile crime during recent years in a unique way. She looked at two variables on a state-wide basis: Supplemental Security Income (SSI) rates for mental health conditions in youth (which can be a proxy for psychiatric medication use) and number of Special Education services. Increased Special Education services in a state was strongly related to declines in juvenile violence, while the number of children on SSI for mental health showed a weak or no correlation with declines in crime. The key point here is that there was no evidence that increased psychiatric treatment in youth led to higher rates of violent crime. In 2006, a small study of 60 male psychotic inpatients hospitalized at a forensic psychiatric unit due to violence had a 75% lower rate of violence toward others after release from the hospital if they remained compliant with their antipsychotic medication. Even more reliable information comes from Big Data studies of the individual medication classes, which are presented in the following sections.
Stimulants
In addition to their well-known effects on reducing impulsivity and inattention in people with ADHD, stimulants also reduce the amount of aggressive and antisocial behavior that some with ADHD (especially those with other psychiatric disorders) are prone to display. In a classic paper published over two decades ago, Dan Connor and his colleagues at the University of Massachusetts Medical School reviewed 28 studies that examined the effect of stimulant medication on aggressive behavior. Nearly 700 children and adolescents participated in these short-term studies. The mean effect size was 0.84 for overt aggression. (See my article “Why We Must Treat ADHD” for a definition of effect size.) For now, it is enough to know that the stimulants were very effective (almost the same effect size that an antibiotic has for a bacterial infection). In another classic study, 22 boys with ADHD were placed in a room by themselves with toys and told to complete a worksheet for which they could earn a reward. The answer sheet was “accidently” left behind in the room. The boys did the task both on placebo and on methylphenidate (Ritalin). While on stimulant, the boys stole the toys in the room less often than on placebo, while they peeked at the answer sheet more often when on stimulant relative to placebo. This showed that medication treatment of ADHD influenced moral reasoning and behavior. Paul Lichtenstein and his colleagues obtained information on 25,656 patients with a diagnosis of ADHD, their pharmacologic treatment, and subsequent criminal convictions in Sweden over five years. They examined the crime rates of these patients in periods in which they were on stimulants compared to when they were not. Medication reduced criminality by 32% in men and 41% in women, an effect seen for both violent and non-violent crime!
Anti-psychotics and Mood Stabilizers
Conclusions from the previously reported study of the effect of anti-psychotic medications on recidivism rates in forensic patients was limited by its small sample size. Zheng Chang and colleagues studied the prescription rates of several classes of medications (antipsychotics, antidepressants, psychostimulants, drugs used in addictive disorders, and
antiepileptic drugs) in 22,275 prisoners released from jail in Sweden, following them for a mean of 4.6 years. Antipsychotic drugs reduced violent crime by 58%, stimulants by 62% and drugs for addictive disorders by 48%. Antidepressants and anti-epileptic drugs did not have any effect on crime. These results were consistent with the results of an earlier study of over 40,000 Swedish men convicted of a violent crime. Those released prisoners who remained on anti-psychotics or mood stabilizing medication had a 45% lower rate of subsequent violent offences. Anti-psychotic medications do carry significant health side effects (e.g., tremors, tardive dyskinesia and cardiovascular risks) but increasing violence is not among them. It seems clear that for those with psychotic or severe mood disorders, anti-psychotics prevent violence.
Antidepressants
Since the “Prozac Defense” emerged in the 1990’s, there has been a concern regarding the possible effects of specific serotonin reuptake inhibitors (SSRIs) on aggressive behavior. This was compounded by the finding that emerged in the early 2000’s from studies of antidepressants in youth with depression in which there was a small, but statistically significant, increase in the rate of suicidal ideation (but not completed suicide) when study participants were on active drug relative to placebo. This led to the “Black Box” warning that is now on the FDA label for all antidepressant medications, stating that there is an “Increased risk of suicidal thinking and behavior in children, adolescents, and young adults taking antidepressants for Major Depressive Disorder (MDD) and other psychiatric disorders.” It is important to look at the issue of suicidal ideation and violence separately rather than conflating these two phenomena, as this often happens in media discussions.
The data on suicidal ideation when antidepressants are used in youth can be difficult to parse, as one needs to look at both short-term and long-term studies. Short-term data comes from the randomized controlled trials comparing antidepressants to placebo; these studies generally last 6-8 weeks. In 2007, Jeffrey Bridge and his colleagues published a review of all the known controlled trials that were done in youth between 1988 and 2006, not only with depression (n = 3,430) but with anxiety (n =1,162) and obsessive-compulsive disorders (OCD, n = 718) as well. They looked at the response rates (how effective the antidepressant was) and the rates of suicidal ideation. Importantly, there was NO completed suicides in any of these trials. The results are shown in the table below:
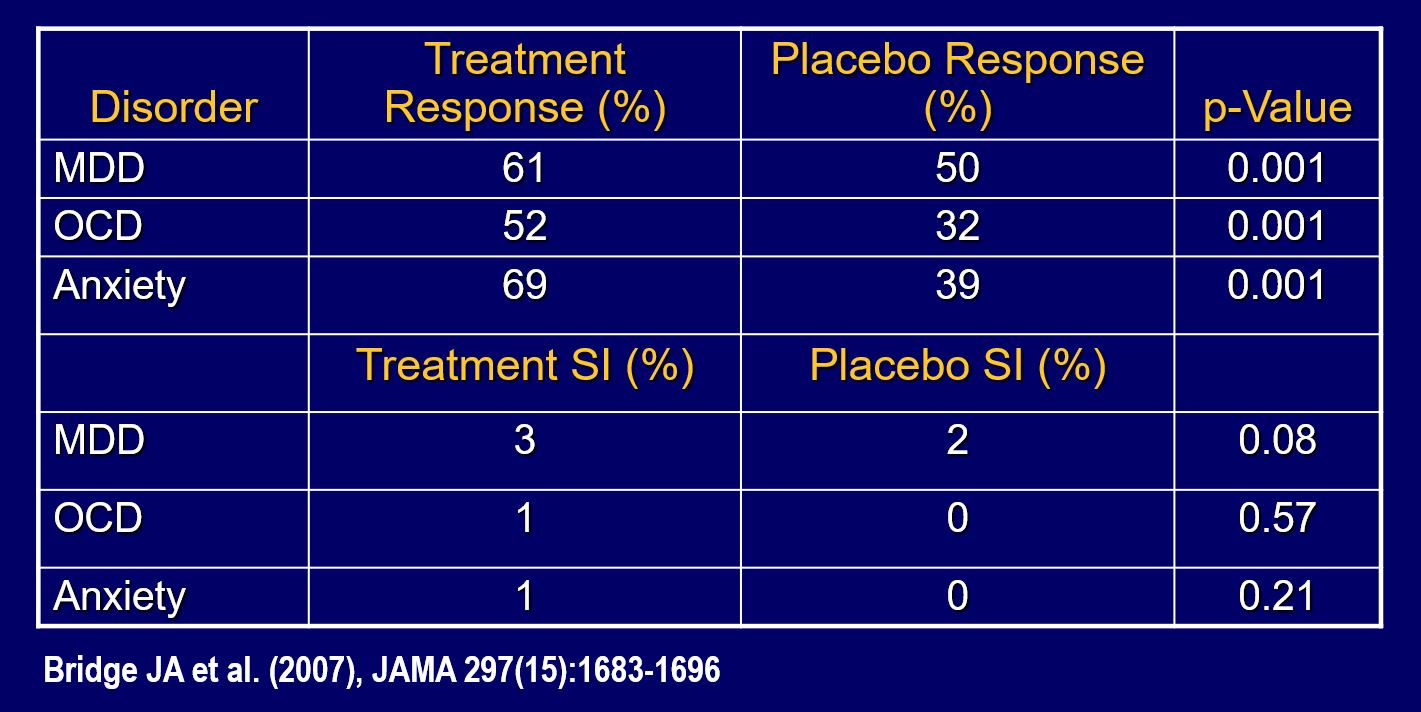
For all three conditions (depression, anxiety and OCD), antidepressants were superior to placebo. The rate of suicidal ideation was very slightly increased (and just missed statistical significance) in youth with depression on antidepressant relative to placebo, but not in the participants with anxiety or OCD.
When this controversy erupted early in the first decade of the 21st century, families and clinicians were concerned and this led to a drop in antidepressant prescription rates. If there were an even modest effect of antidepressants to increase suicidal rates, then one would have expected a decline in the number of completed suicides. The opposite occurred. Suicide rates had declined in the period 1990-2002 as antidepressants prescriptions in youth increased, followed by an immediate increase of 2.07 suicides per 100,000 youth in the period after the Black Box Warning. Moreover, a county-by-county analysis in the U.S. found that the more prescriptions given for antidepressants, the lower the suicide rate. As I discussed in my posts on the Youth Mental Health Crisis, suicide rates have been rising again in the last decade despite increasing rates of antidepressant prescriptions to youth, showing that there is no simple relationship between completed sucide and antidepressants.
Results regarding antidepressants and violent or aggressive behavior also need to be parsed carefully. Nationwide data from the Netherlands in 2012 showed a significant effect of antidepressants to reduce lethal violence, while a study of SSRIs in a Swedish cohort found a modest effect of SSRIs on violent crime, and only in the persons aged 15 to 24 years. Tyra Lagerberg and colleagues identified individuals aged 15–60 years (n = 785,337) who were ever dispensed a SSRI in Sweden during the years 2006–2013. The investigators linked SSRI prescription status (on vs. off medication) to records of violent crime. For those on an SSRI, 97% did not commit a violent crime. However, rates of violent offences were higher in 15-34 year-olds on SSRI but not in older persons. There was evidence that a small number (2.6%) of SSRI users were more likely to commit an act of violence while on the SSRI. On the other hand, a small study of 53 youth with severe mood dysregulation (and high aggression) showed modest improvement on an SSRI (35% improved) relative to placebo (6% improved). No agitation or aggression was seen as a side effect in the trial.
Given the preponderance of the data, we can conclude that antidepressants are safe and effective for youth mood and anxiety disorders, although there may be a very small subset who are vulnerable to either experience suicidal ideation or have an aggressive outburst. There is no evidence that such phenomena plays a role in mass shootings. Can we reconcile the conflicting findings? Imagine 100 youth with depression who go untreated. Some will improve naturally, and others will deteriorate so that within a period of a year, 60 youth remain depressed, one person becomes violent, five commit suicide and around forty improve. Imagine now that 100 depressed youth are started on an antidepressant. Two experience new suicidal ideation in the first three weeks they are treated but it resolves. Three individuals get agitated and need to be taken off the antidepressant. One year later, 60 people are improved in terms of depression and only one has committed suicide. Thus, you can see that despite some short-term mood effects, the sample overall does better if they are treated than if they are not. This would explain why over time, communities with more treated individuals have lower suicide rates.
Defending the Benefits of Psychiatric Medications
We may be entering a difficult time in which unorthodox and fringe medical beliefs may become more prominent in the years ahead. While much of the distrust in science has to this point been aimed at vaccines, those concerned about mental health should be on guard that access to life-saving psychiatric medications may be challenged. The facts are on our side, however, and it is time to advocate aggressively for our patients.